Clinical History: A 4-year-old boy presented to his pediatrician with a one-week history of a swollen, tender left knee, fever and chills following a fall at the playground. A plain radiograph was obtained and blood cultures were taken. Antibiotics were given; however, since the condition did not resolve, a bone biopsy was performed.
This is a plain radiograph that shows AP and lateral views of the distal lower extremity. The epiphyses are open, consistent with the patients age. There is a diffuse process involving the tibia from the distal epiphysis to the proximal metaphysis. The appearance suggests an aggressive process due to the moth-eaten appearance. The periosteum appears to be significantly lifted from the bone this can be seen, particularly in young children, resulting in subperiosteal abscesses..
Sections show fragments of bone with osteonecrosis the lacunae do not have osteocytes. There is an associated brisk acute inflammatory infiltrate composed primarily of neutrophils. Plasma cells are present in the fibrotic areas. Dark purple granular bacterial colonies are focally present.
Webslide 0301, developing finger, long. sect.
[ImageScope]
[WebScope]
The bones shown in Webslide 301 (distal end of a metacarpal, and the 1st, 2nd, and part of the 3rd phalangeals) are still undergoing the process of endochondral ossification, but there are many general features of long bones that can be appreciated. The shaft of each bone (the diaphysis) consists of a rigid cylinder of compact bone (example) surrounding a hollow marrow cavity (example). Within the marrow cavity are hematopoietic cells and some adipocytes amongst spicules of trabeculated, or spongy, bone. As most long bones mature, the hematopoietic cells are replaced by the adipocytes and the marrow transitions from being 'red' (hematopoietic) to 'yellow' (fatty).
Outside of the cylinder of compact bone is a connective tissue sheath known as the periosteum. The periosteum is further subdivided into an inner, cellular periosteum (close to the bone), which is less dense in nature and made up of fibroblasts and osteoprogenitor cells and an outer, fibrous periosteum made up of dense, irregular connective tissue. The periosteum adheres to the bone by way of Sharpey's fibers that extend from the fibrous layer into the compact bone (example).
The articular surfaces at the ends of the bones (the epiphyses) are comprised of hyaline cartilage. Active growth plates (or epiphyseal plates) may be observed at the proximal ends of the phalanges (example) and the distal end of the metacarpal bone (example) whereas the cartilage at the distal ends of the phalanges exhibits much less proliferation (example), which is consistent with the general pattern of growth observed these and other long bones.
050_HISTO_40X, fibula, cross sect.
[ImageScope]
[WebScope]
This is a cross section of a fibula from an adolescent primate and therefore exhibits characteristics of more mature bone. The marrow cavity still contains a great deal of hematopoietic cells and would therefore be considered ‘red’ --however, note that there is a significant amount of adipose tissue that will increase over time. The shaft of the fibula consists of compact bone which is organized into inner (example) and outer (example) circumferential lamella, made up of bone laid down in concentric layers. Sandwiched between the inner and outer lamellae are collections of osteons, or Haversian systems (example). Within the bone, you can see the individual osteocytes within their lacunae and the small canaliculi through which the osteocytes extend processes to communicate with each other. The periosteum is relatively thin and consists primarily of an outer fibrous layer of dense irregular connective tissue. Outside the periosteum are fibers of skeletal muscle associated with the extensor and flexor compartments of the leg.
510-4. A 15-year-old boy is diagnosed with osteomyelitis of the left tibia. Cultures are positive for Salmonella typhi. This patient most likely has which of the following?
Clinical History: A 13-year-old boy presented to his pediatrician with a 6-week history of left knee pain and swelling. A plain radiograph was obtained.
This plain radiograph shows open epiphyses, consistent with the patients age. There is a destructive metaphyseal tumor with a moth-eaten appearance (ie. aggressive features). A soft tissue density that appears to be partially calcified can be appreciated.
Webslide 0301, developing finger, long. sect.
[ImageScope]
[WebScope]
The bones shown in Webslide 301 (distal end of a metacarpal, and the 1st, 2nd, and part of the 3rd phalangeals) are still undergoing the process of endochondral ossification, but there are many general features of long bones that can be appreciated. The shaft of each bone (the diaphysis) consists of a rigid cylinder of compact bone (example) surrounding a hollow marrow cavity (example). Within the marrow cavity are hematopoietic cells and some adipocytes amongst spicules of trabeculated, or spongy, bone. As most long bones mature, the hematopoietic cells are replaced by the adipocytes and the marrow transitions from being 'red' (hematopoietic) to 'yellow' (fatty).
Outside of the cylinder of compact bone is a connective tissue sheath known as the periosteum. The periosteum is further subdivided into an inner, cellular periosteum (close to the bone), which is less dense in nature and made up of fibroblasts and osteoprogenitor cells and an outer, fibrous periosteum made up of dense, irregular connective tissue. The periosteum adheres to the bone by way of Sharpey's fibers that extend from the fibrous layer into the compact bone (example).
The articular surfaces at the ends of the bones (the epiphyses) are comprised of hyaline cartilage. Active growth plates (or epiphyseal plates) may be observed at the proximal ends of the phalanges (example) and the distal end of the metacarpal bone (example) whereas the cartilage at the distal ends of the phalanges exhibits much less proliferation (example), which is consistent with the general pattern of growth observed these and other long bones.
050_HISTO_40X, fibula, cross sect.
[ImageScope]
[WebScope]
This is a cross section of a fibula from an adolescent primate and therefore exhibits characteristics of more mature bone. The marrow cavity still contains a great deal of hematopoietic cells and would therefore be considered ‘red’ --however, note that there is a significant amount of adipose tissue that will increase over time. The shaft of the fibula consists of compact bone which is organized into inner (example) and outer (example) circumferential lamella, made up of bone laid down in concentric layers. Sandwiched between the inner and outer lamellae are collections of osteons, or Haversian systems (example). Within the bone, you can see the individual osteocytes within their lacunae and the small canaliculi through which the osteocytes extend processes to communicate with each other. The periosteum is relatively thin and consists primarily of an outer fibrous layer of dense irregular connective tissue. Outside the periosteum are fibers of skeletal muscle associated with the extensor and flexor compartments of the leg.
223-1. Based on the clinical history and findings thus far, what is the differential diagnosis?
Webslide 0301, developing finger, long. sect.
[ImageScope]
[WebScope]
The bones shown in Webslide 301 (distal end of a metacarpal, and the 1st, 2nd, and part of the 3rd phalangeals) are still undergoing the process of endochondral ossification, but there are many general features of long bones that can be appreciated. The shaft of each bone (the diaphysis) consists of a rigid cylinder of compact bone (example) surrounding a hollow marrow cavity (example). Within the marrow cavity are hematopoietic cells and some adipocytes amongst spicules of trabeculated, or spongy, bone. As most long bones mature, the hematopoietic cells are replaced by the adipocytes and the marrow transitions from being 'red' (hematopoietic) to 'yellow' (fatty).
Outside of the cylinder of compact bone is a connective tissue sheath known as the periosteum. The periosteum is further subdivided into an inner, cellular periosteum (close to the bone), which is less dense in nature and made up of fibroblasts and osteoprogenitor cells and an outer, fibrous periosteum made up of dense, irregular connective tissue. The periosteum adheres to the bone by way of Sharpey's fibers that extend from the fibrous layer into the compact bone (example).
The articular surfaces at the ends of the bones (the epiphyses) are comprised of hyaline cartilage. Active growth plates (or epiphyseal plates) may be observed at the proximal ends of the phalanges (example) and the distal end of the metacarpal bone (example) whereas the cartilage at the distal ends of the phalanges exhibits much less proliferation (example), which is consistent with the general pattern of growth observed these and other long bones.
050_HISTO_40X, fibula, cross sect.
[ImageScope]
[WebScope]
This is a cross section of a fibula from an adolescent primate and therefore exhibits characteristics of more mature bone. The marrow cavity still contains a great deal of hematopoietic cells and would therefore be considered ‘red’ --however, note that there is a significant amount of adipose tissue that will increase over time. The shaft of the fibula consists of compact bone which is organized into inner (example) and outer (example) circumferential lamella, made up of bone laid down in concentric layers. Sandwiched between the inner and outer lamellae are collections of osteons, or Haversian systems (example). Within the bone, you can see the individual osteocytes within their lacunae and the small canaliculi through which the osteocytes extend processes to communicate with each other. The periosteum is relatively thin and consists primarily of an outer fibrous layer of dense irregular connective tissue. Outside the periosteum are fibers of skeletal muscle associated with the extensor and flexor compartments of the leg.
223-2. Which of the following is the most common site of origin of these tumors?
223-3. Mutations and loss of function of the RB and P53 genes are commonly seen in this disease process. These two genes are examples of which of the following?
Clinical History: A 16-year-old boy presented to the pediatrician with a 1-month history of pain and swelling of the left hip. He told the pediatrician that he had been struck there by a baseball four months earlier. Plain radiography and MRI were performed, followed by a needle biopsy. Neoadjuvant chemotherapy was given prior to limb-salvage surgery.
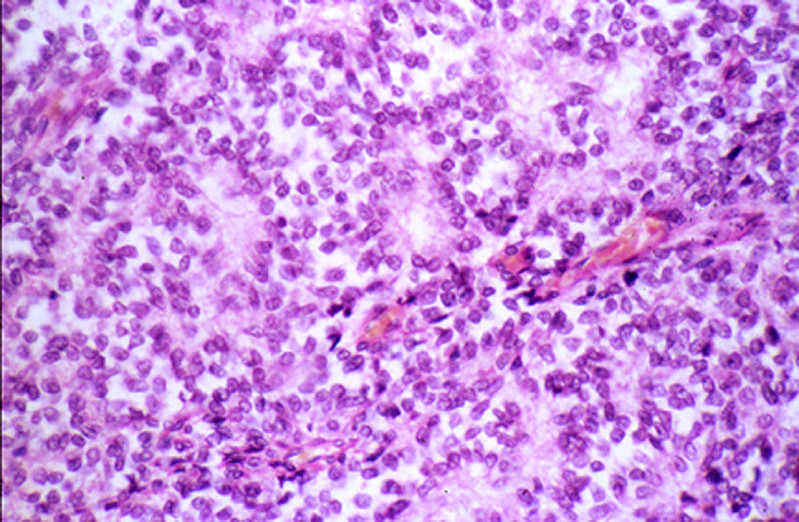
The radiograph shows a lytic, infiltrative lesion in the proximal half of the femur. There are reactive periosteal changes in the proximal diaphysis with an onion-skin appearance. The MRI shows the tumor extending into the soft tissue. Cross section through the resected femoral head shows a soft tan white tumor with focal hemorrhage and necrosis. There is extensive soft tissue invasion.
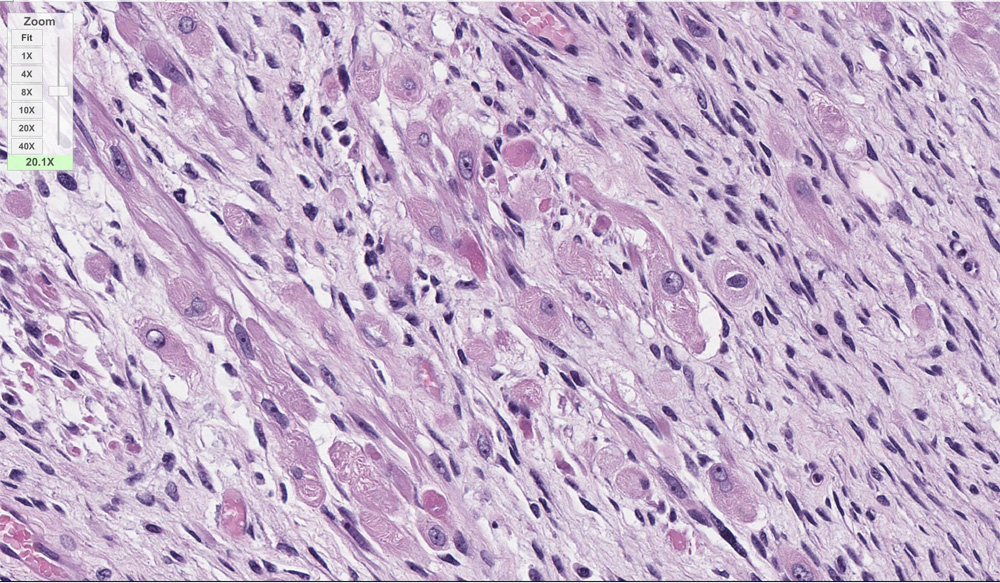
A striking feature is the monotony of the cells with round to oval vesicular nuclei and poorly defined, scanty eosinophilic cytoplasm. There are a moderate number of mitoses, but tumor giant cells and pleomorphism are conspicuously absent. The tumor cells are arranged around scanty, very vascular, fibrous stroma in a trabecular fashion, sometimes resembling rosette formation. In between these cords the tumor cells seem to line empty spaces. Histologically it is quite difficult to distinguish this tumor from a neuroblastoma.
Webslide 0301, developing finger, long. sect.
[ImageScope]
[WebScope]
The bones shown in Webslide 301 (distal end of a metacarpal, and the 1st, 2nd, and part of the 3rd phalangeals) are still undergoing the process of endochondral ossification, but there are many general features of long bones that can be appreciated. The shaft of each bone (the diaphysis) consists of a rigid cylinder of compact bone (example) surrounding a hollow marrow cavity (example). Within the marrow cavity are hematopoietic cells and some adipocytes amongst spicules of trabeculated, or spongy, bone. As most long bones mature, the hematopoietic cells are replaced by the adipocytes and the marrow transitions from being 'red' (hematopoietic) to 'yellow' (fatty).
Outside of the cylinder of compact bone is a connective tissue sheath known as the periosteum. The periosteum is further subdivided into an inner, cellular periosteum (close to the bone), which is less dense in nature and made up of fibroblasts and osteoprogenitor cells and an outer, fibrous periosteum made up of dense, irregular connective tissue. The periosteum adheres to the bone by way of Sharpey's fibers that extend from the fibrous layer into the compact bone (example).
The articular surfaces at the ends of the bones (the epiphyses) are comprised of hyaline cartilage. Active growth plates (or epiphyseal plates) may be observed at the proximal ends of the phalanges (example) and the distal end of the metacarpal bone (example) whereas the cartilage at the distal ends of the phalanges exhibits much less proliferation (example), which is consistent with the general pattern of growth observed these and other long bones.
050_HISTO_40X, fibula, cross sect.
[ImageScope]
[WebScope]
This is a cross section of a fibula from an adolescent primate and therefore exhibits characteristics of more mature bone. The marrow cavity still contains a great deal of hematopoietic cells and would therefore be considered ‘red’ --however, note that there is a significant amount of adipose tissue that will increase over time. The shaft of the fibula consists of compact bone which is organized into inner (example) and outer (example) circumferential lamella, made up of bone laid down in concentric layers. Sandwiched between the inner and outer lamellae are collections of osteons, or Haversian systems (example). Within the bone, you can see the individual osteocytes within their lacunae and the small canaliculi through which the osteocytes extend processes to communicate with each other. The periosteum is relatively thin and consists primarily of an outer fibrous layer of dense irregular connective tissue. Outside the periosteum are fibers of skeletal muscle associated with the extensor and flexor compartments of the leg.
Clinical History: A 62-year-old white farmer presented to his primary care physician with a 3-year history of a slowly growing lesion on his right temple. The lesion was excised.
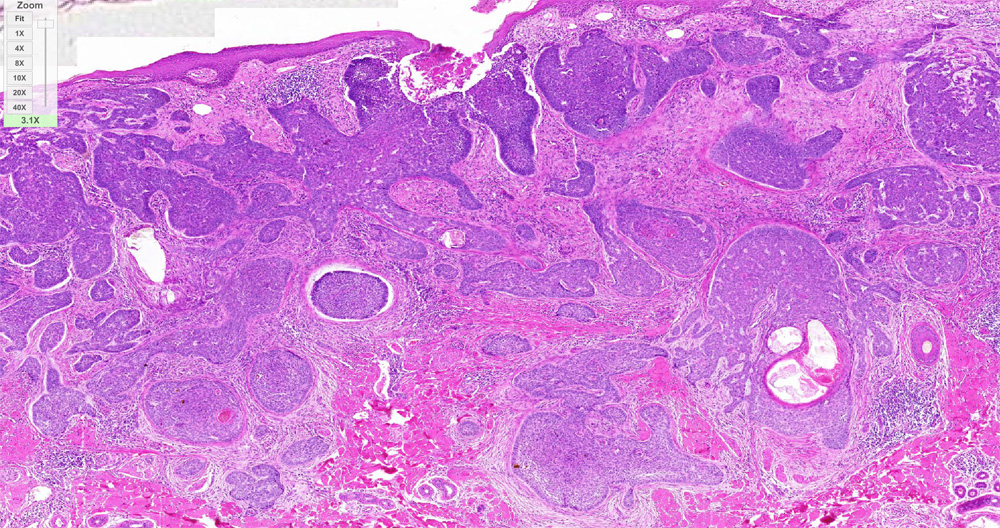
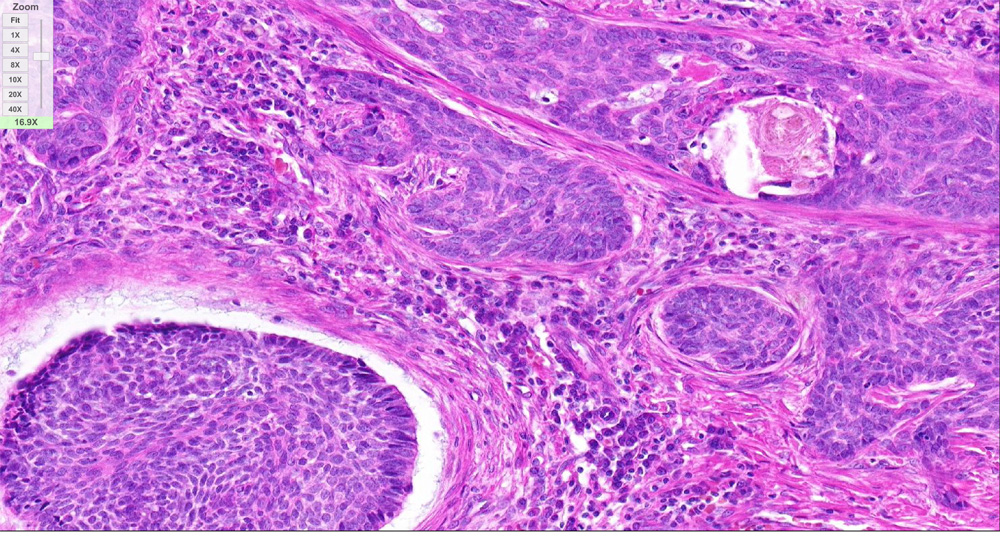
There was a well circumscribed, firm, elevated mass 1cm in diameter. The overlying skin was intact but smooth and has a pearly, pink appearance. There is central umbilication.
There are nests of darkly staining basophilic cells in the upper dermis with peripheral palisading. There is little cytoplasm, and the cytoplasmic borders are poorly defined. Nuclei are small and are round or oval, and occasional apoptotic bodies are noted. These tumors may arise from the basal cell layer of the epidermis or from dermal appendages. In this particular tumor there is an occasional round mass of keratin which is not usually seen in basal cell carcinomas. Note the loose, myxoid stroma about the tumor cells with some artefactual clefts.
Skin consists of keratinizing stratified squamous epithelium. The keratin layer is eosinophilic. Nuclei are not present. Beneath the keratin layer is a layer of flat epithelial cells with small pyknotic nuclei. Cells are regular and not crowded. These keratinocytes rest upon a layer of basal epithelium and a thin basement membrane. Beneath the epidermis is the dermis which consists of loose connective tissue. Within the dermis are sweat and sebaceous glands. Some slides contain hair follicles. There is no inflammation. The blood vessels are patent and do not contain thromboemboli.
There is marked epidermal hyperplasia with a papillated surface, thickening of the granular layer (hypergranulosis) and cornified layer (hyperkeratosis). Within the granular layer, many of the cells contain large, coarse keratohyalin granules. There are foci of preservation of nuclei in the cornified layer (parakeratosis), especially overlying the tips of the papillae. The vessels in the papillary dermis are dilated.
Skin consists of keratinizing stratified squamous epithelium. The keratin layer is eosinophilic. Nuclei are not present. Beneath the keratin layer is a layer of flat epithelial cells with small pyknotic nuclei. Cells are regular and not crowded. These keratinocytes rest upon a layer of basal epithelium and a thin basement membrane. Beneath the epidermis is the dermis which consists of loose connective tissue. Within the dermis are sweat and sebaceous glands. Some slides contain hair follicles. There is no inflammation. The blood vessels are patent and do not contain thromboemboli.
Clinical History: A 45-year-old man presented to his primary care physician with a 2-week history of a bleeding lesion on the back. His wife noticed that the lesion seemed to have been growing over the past several months. The primary care physician suspected a vascular lesion and referred him to the dermatology department for a biopsy.
The sections show a compound proliferation of atypical melanocytes involving the epidermis and dermis. Ulceration is noted in the epidermis (absence of epidermis with collection of serum and inflammation). The severely atypical melanocytes are arranged as single cells and nests in the epidermis with focal pagetoid spread. The dermis is distended by melanocytes lacking maturation (cells do not decrease in size from papillary to reticular dermis). High power view of the melanocytes show abundant eosinophilic cytoplasm, with high N/C ratio and prominent nucleoli. Mitotic figures are seen.
Skin consists of keratinizing stratified squamous epithelium. The keratin layer is eosinophilic. Nuclei are not present. Beneath the keratin layer is a layer of flat epithelial cells with small pyknotic nuclei. Cells are regular and not crowded. These keratinocytes rest upon a layer of basal epithelium and a thin basement membrane. Beneath the epidermis is the dermis which consists of loose connective tissue. Within the dermis are sweat and sebaceous glands. Some slides contain hair follicles. There is no inflammation. The blood vessels are patent and do not contain thromboemboli.
Clinical History: A 6-month-old girl was brought to the emergency department with a 1-month history of a vaginal growth and vaginal bleeding. Her parents mentioned that her abdomen had appeared swollen for the last two weeks. Physical exam revealed a suprapubic, mobile mass and an erythematous mass protruding from the vagina. Laboratory tests were noncontributory. A biopsy was performed.
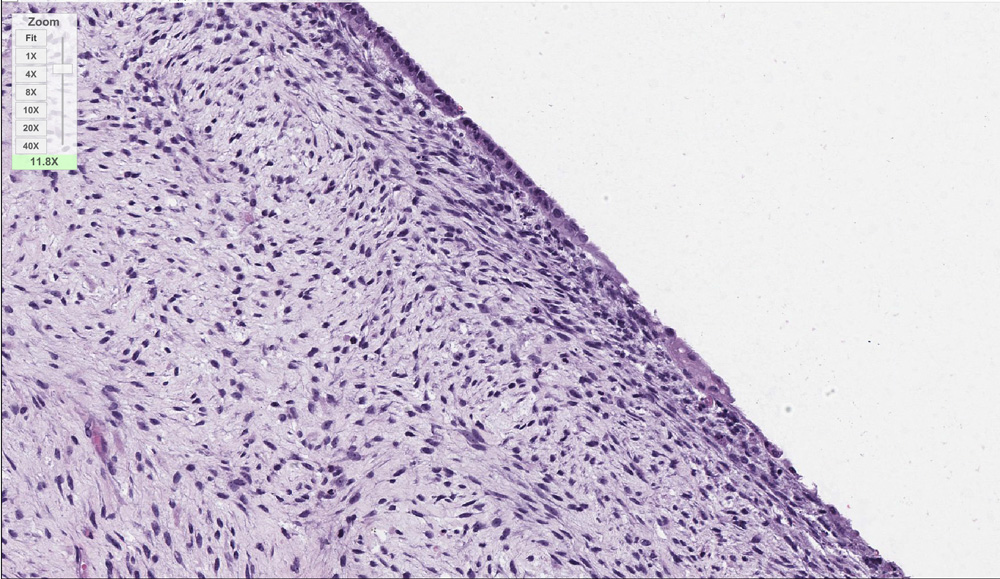
Endocervical mucosa overlies a proliferation of spindle cells in a loose, myxoid stroma that modulates from areas of greater to lower cell density. There are collections of rhabdomyoblasts (primitive skeletal muscle cells) with abundant eosinophilic cytoplasm. Strap cells and primitive myotubules are also present. Beneath the epithelium, there is a linear condensation of spindle cells to form a cambium layer (as seen in the 3rd microscopic image in the image gallery). Mitotic activity is low. Atypical mitotic figures, necrosis and anaplasia are not seen.
This slide spans the boundary between the uterine cervix and the vagina.
First, scan at low power the cervix on the lower edge of the section and observe the cervical glands in the endometrium. Notice that the large, branched glands differ in shape from the glands in most of the uterus (previous slides). Unlike in the rest of the uterus, the endometrium in the cervix changes little in thickness during the menstrual cycle. Much of the cervical surface epithelium is not present in this slide, but you should be able to identify the simple columnar epithelium cells lining the cervical glands that secrete mucus serving to lubricate the vagina. The myometrium contains bundles of smooth muscle, and the simple squamous mesothelium covering the perimetrium is evident in your slide.
Although the epithelium at the boundary of the cervix and vagina is not preserved, the non-keratinized stratified squamous epithelium of the vagina is present at the right hand surface of the slide. The outer layers of these epithelial cells are filled with glycogen giving them an empty appearance, characteristic of this vaginal epithelium. The vaginal mucosa is highly vascularized, but contains no glands. The ill-defined muscle layers contain bundles of smooth muscle. The muscle layers grade into an adventitia.
Absolutely critical information you must know to practice medicine is in bold font. Important information that will be needed for routine patient care is in regular font. Information about less common diseases that you may encounter in clinical practice and that will probably appear on examinations is in italics
Discuss the following hereditary disorders, in terms of pathogenesis, morphology, and clinical presentation:
Describe the morphologic sequence of normal bone growth, as well as of repair following fracture of a long bone. Indicate the way(s) in which age, mobility, nutritional state, and infection influence the repair process.
Discuss the following non‑neoplastic bone disorders, in terms of etiology, pathogenesis, morphology, and clinical findings and course:
Absolutely critical information you must know to practice medicine is in bold font. Important information that will be needed for routine patient care is in regular font. Information about less common diseases that you may encounter in clinical practice and that will probably appear on examinations is in italics
Compare and contrast the clinical and pathologic features of :